
The diversity of the T cell repertoire allows for recognition of a wide diversity of pathogens. During T cell development, T cell receptors (TCRs) undergo genetic rearrangements of their V, D, and J segments, as well as random deletions and nontemplated additions of nucleotides. Furthermore, major histocompatibility complex (MHC) class I and II molecules are highly polymorphic. Thus, each person has a unique and highly diverse T cell-MHC repertoire. In addition, there are two known classes of lymphocytes with restricted diversity of their TCR α-chains, and which bind to the non/rarely polymorphic antigen-presenting molecule families CD1 and MR1. These are the invariant natural killer T cells (iNKT cells), and the mucosa-associated invariant T cells (MAIT cells), respectively. In the June issue of Nature Immunology, Van Rhijn et al. identify a new class of T cells with restricted TCR α-chains, termed GEM T cells, that recognize the Mycobacterium tuberculosis (Mtb) lipid glucose monomycolate presented on CD1b.
To study the human TCR repertoire recognizing CD1b, Van Rhijn et al., utilized CD1b tetramers loaded with glucose monomycolate (GMM), to isolate and clone T cells from peripheral blood mononuclear cells (PBMC) of Mtb infected donors. Two groups of T cell clones with differing avidity for CD1b-GMM were isolated from each patient, differentiated by intermediate (CD1bint) and high (CD1bhi) CD1b tetramer staining intensities. CD1bint T cells were diverse in their TCR α-chain sequences. TCR α-chains of CD1bhi T cells however, all utilized the same variable and joining sequences (TRAV1-2, and TRAJ9, respectively) with few nontemplated additions, resulting in a specific complementarity-determining region 3 (CDR3) consensus sequence. Thus, these were termed “germline-encoded, mycolyl lipid–reactive” (GEM) T cells. These TCR α-chain sequences furthermore had to be paired with specific TCR β-chain sequences in order to recognize CD1b-GMM complexes.
Other properties of these uniquely identified GEM T cells included expression of CD4 and production of IFNγ and TNFα upon activation, two cytokines important for anti-mycobacterial responses. GEM T cells expressed various rates of CD161, a marker widely expressed by NKT cells and MAITs, and thus GEM T cells could not be defined by expression of CD161. In addition, sorting of TRAV1-2+ CD4+ cells from two healthy donors followed by deep sequencing of the TCR α-chain revealed identification of the GEM-specific CDR3 sequence, demonstrating that GEM T cells were present in Mtb uninfected individuals in the naïve T cell repertoire. However, these cells become clonally expanded in Mtb infected patients, and thus likely to contribute to anti-mycobacterial immune responses.
In conclusion, GEM T cells are a newly identified third class of CD1-recognizing T cells with restricted TCR α-chain sequences. These cells arise via VDJ recombination, and indicate that special selection mechanisms exist to generate T cells bearing this specific TCR α-chain. Although what CD1b-self antigen complex could positively select for these cells in the thymus is unknown. Furthermore, the role these cells play during mycobacterial infections will be an interesting avenue for future studies.
Further Reading:
A conserved human T cell population targets mycobacterial antigens presented by CD1b. Van Rhijn I, Kasmar A, de Jong A, Gras S, Bhati M, Doorenspleet ME, de Vries N, Godfrey DI, Altman JD, de Jager W, Rossjohn J, Moody DB. Nat Immunol. 2013 Jun 2;14(7):706-13.
A ‘GEM’ of a cell. Mitchell Kronenberg & Dirk M Zajonc. Nature Immunology 14, 694–695 (2013) doi:10.1038/ni.2644. Published online 18 June 2013.












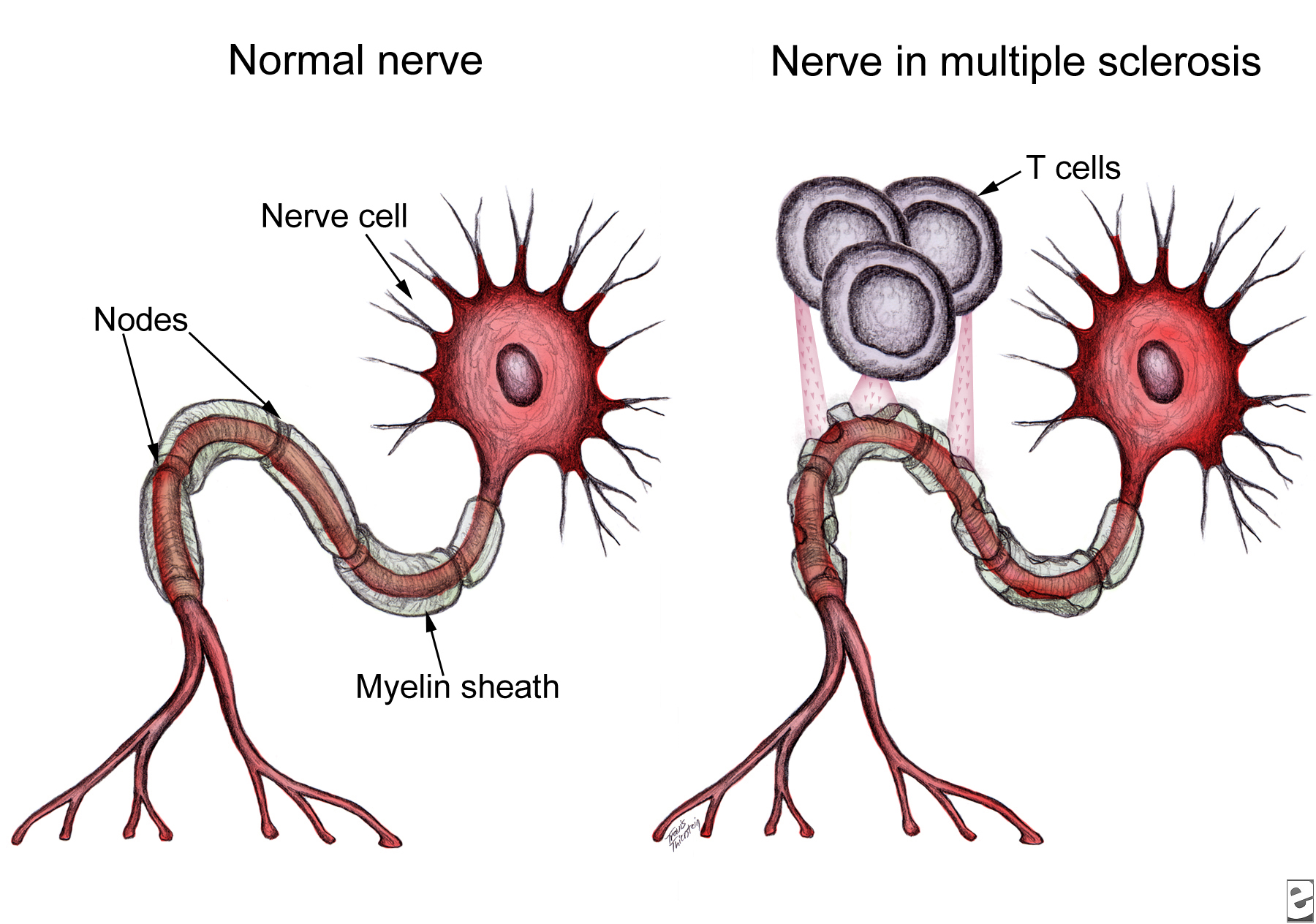

 These results support the epitope-spreading hypothesis, which indicates that MS patients make antibodies against one or a few myelin proteins, but as the disease progresses, the autoimmune response spreads to other myelin sheath epitopes. In their recent publication, Lutterotti et al. provide sufficient evidence necessitating emphasis not only on the specific target antigens, but also on the facility to inhibit epitope spreading, preferably prior to diversification of the
These results support the epitope-spreading hypothesis, which indicates that MS patients make antibodies against one or a few myelin proteins, but as the disease progresses, the autoimmune response spreads to other myelin sheath epitopes. In their recent publication, Lutterotti et al. provide sufficient evidence necessitating emphasis not only on the specific target antigens, but also on the facility to inhibit epitope spreading, preferably prior to diversification of the 